"Although glaucoma implants are increasingly being used as a primary surgical option in the USA and Europe, their most common indication remains refractory glaucomas—such as neovascular glaucomas, which often occur in patients with diabetes or venous thrombosis, and glaucomas in which traditional filtering surgeries have failed, particularly those using antifibrotic agents like mitomycin C or 5-fluorouracil.”
The Implante de Susanna UF is a silicone implant designed to facilitate aqueous humor drainage and reduce intraocular pressure in patients with glaucoma—particularly in refractory cases, or when previous surgeries have failed, or are expected to yield poor results based on clinical experience with conventional filtering procedures.
Refractory glaucomas include neovascular glaucomas, medication-resistant glaucomas, uveitic glaucomas, and pseudophakic glaucomas.
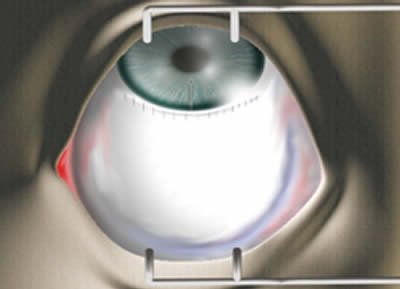
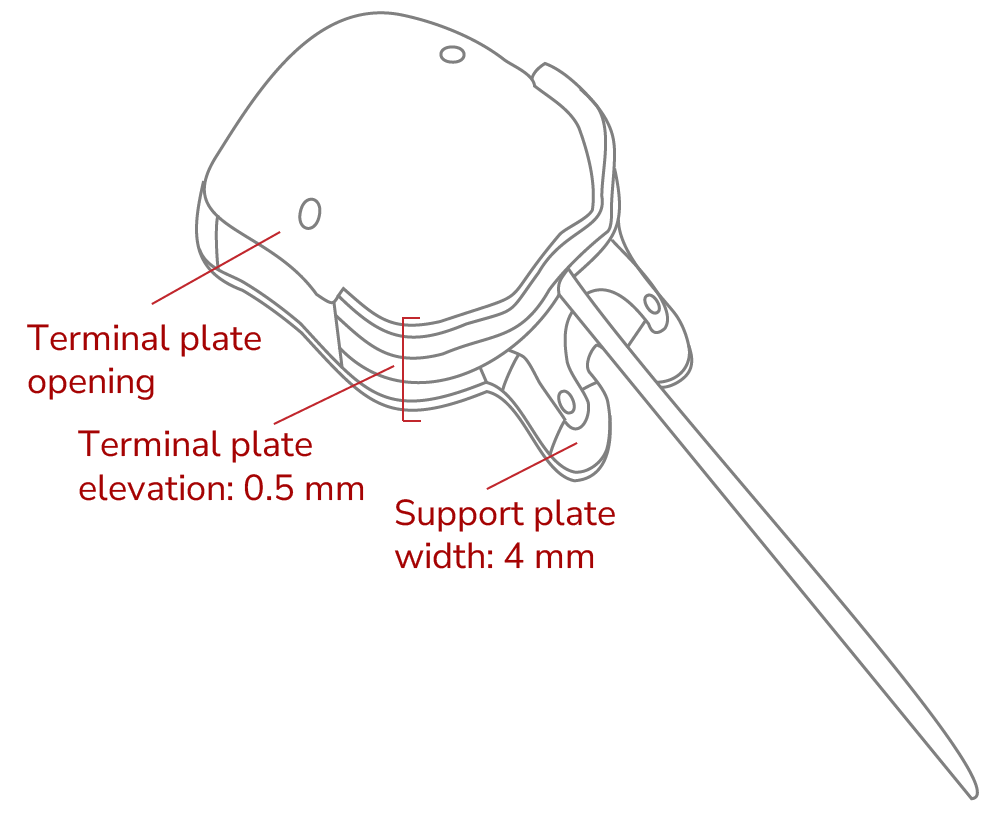
The Implante de Susanna UF consists of a drainage tube and a silicone reservoir (plate). This plate is anatomically contoured to follow the curvature of the globe and features an elevated anterior rim designed to prevent tube blockage by fibrous or conjunctival tissue.
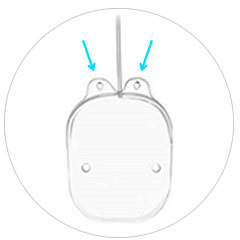
The Implante de Susanna UF features two small anterior fixation feet, each 4 mm long, allowing secure scleral fixation 6 mm from the limbus. This positions the plate 10 mm from the limbus, a site recommended to minimize the risk of extrusion.

Prepare the implant: Attach a 30-gauge cannula connected to a syringe filled with normal saline to the distal end of the drainage tube. Slowly inject 1.0 cc of saline through the implant to confirm patency and verify unobstructed flow.

Make a fornix-based conjunctival incision, dissecting through Tenon’s capsule. Create a sub-Tenon’s pocket in the superior quadrant between the medial and lateral rectus muscles by separating Tenon’s capsule from the episclera.

Insert the implant body into the pocket between the rectus muscles and suture it to the sclera

The anterior edge of the implant should be positioned 8–10 mm from the limbus. To achieve this, the fixation feet must be placed 6 mm from the limbus.

Trim the drainage tube to allow 2–3 mm of insertion into the anterior chamber (AC). The tube should be beveled at an angle of approximately 30° to facilitate insertion.

Perform a paracentesis and enter the AC at the limbus using a 23-gauge needle, advancing parallel to the iris.

Attention: The drainage tube must not touch the iris or corneal endothelium after insertion.

Insert 2–3 mm of the drainage tube into the AC through the tract created by the needle, ensuring it remains parallel to the iris. The leading edge of the implant should be 8–10 mm from the limbus.

Cover the tube with scleral or pericardial patch graft and suture in place, then close the conjunctiva.